An Operation Smile volunteer reverses an oxygen mask so a child with a cleft condition can blow a bubble for the first time in Guadalajara, Mexico. (Operation Smile Photos)
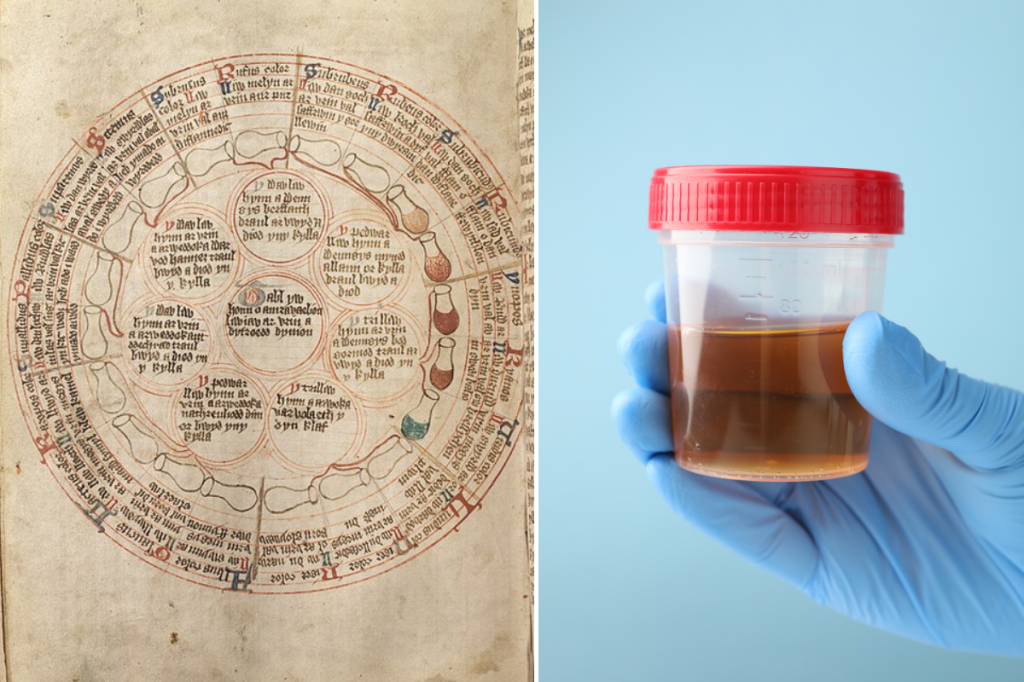
Photo credit: National Library of Wales/Wikimedia Commons & Canva Photos – A guy says he can tell when he's getting sick based on the taste of his pee. Ancient doctors would probably agree.
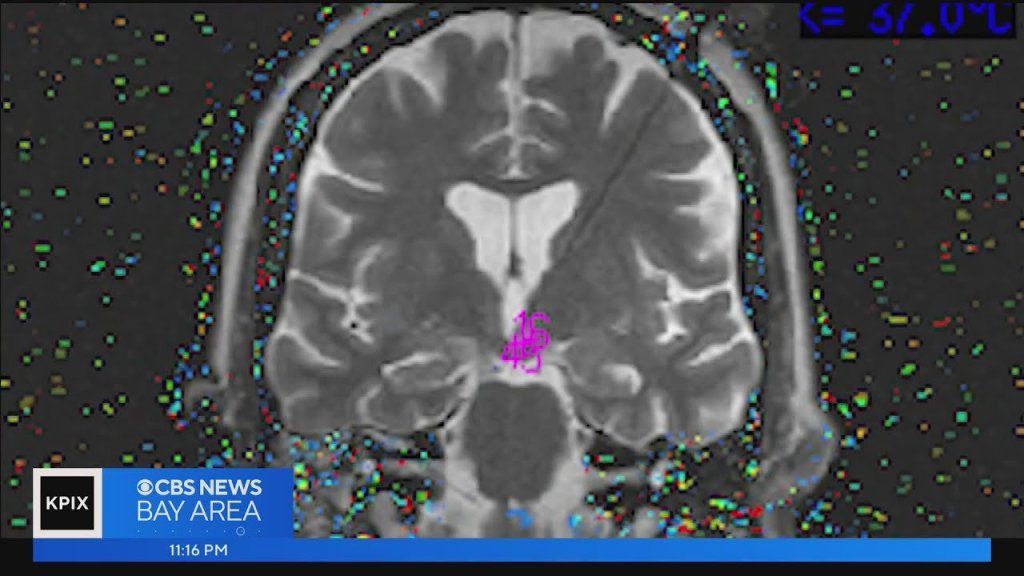
Photo credit: Photo by National Cancer Institute on Unsplash – "Awake surgery" allows brain surgeons to see the functioning parts of the brain to avoid during surgery.













{kind=link}